Key Takeaways
- Treat agency selection as a regulatory audit, since healthcare content must withstand scrutiny from HHS, FTC, federal prosecutors, and clinical reviewers, not just marketing performance review 4, 5, 16, 9.
- Test regulatory fluency across HIPAA marketing authorization, FTC substantiation, EKRA and patient-brokering statutes, and AMA Code 9.6.1, because vague compliance assurances fail under procurement and enforcement review 4, 5, 16, 9.
- Review sample content the way a clinical director would, checking primary literature citations, effect-size accuracy, and documented consent for patient stories rather than relying on marketing polish 3, 5.
- Require agencies to design for multi-channel information triangulation, since 73% of Americans use multiple sources and single-funnel SEO programs miss most of the actual decision path 10, 1.
- Demand measurement reporting that connects acquisition metrics to qualified admissions and CAHPS-style patient-experience signals, so the program reflects delivered care, not just funnel activity 11, 3.
- Verify sector-specific fluency in SAMHSA frameworks for SUD and OTP services and SGIM telehealth standards, since federal rules dictate what can be promised in patient-facing copy 12, 13, 18.
- Run a structured diligence sequence covering pre-RFP document requests, scored work-sample audits, reference calls, and healthcare counsel review before signing any contract 4, 5, 16, 7.
- For multi-facility operators, separate fixed editorial infrastructure from per-location variables like GBP maintenance and call tracking, and confirm BAA coverage for every tracking number 4, 12.
Why Agency Selection Is a Regulatory Audit, Not a Procurement Exercise
Selecting a healthcare content marketing agency is more akin to a compliance audit than a typical procurement decision. The content produced, whether a blog series or landing pages, must withstand scrutiny from various regulatory bodies. This includes the HHS under the HIPAA Privacy Rule 4, the FTC regarding health product substantiation 5, federal prosecutors concerning EKRA and state patient-brokering statutes 16, and the AMA Code of Medical Ethics for physician-involved messaging 9.
This means the true deliverable is not just content, but content that an organization can defend in regulatory reviews, legal depositions, and clinical assessments, while still achieving marketing objectives like increasing admissions and optimizing cost per admission.
Generic agency evaluations often overlook these critical compliance aspects, focusing instead on case studies, traffic metrics, and team chemistry. While these factors are important, they are secondary to an agency’s ability to produce work that adheres to the evidentiary, ethical, and privacy standards governing healthcare promotion 3. An agency unable to provide documentation for these standards represents a significant liability.
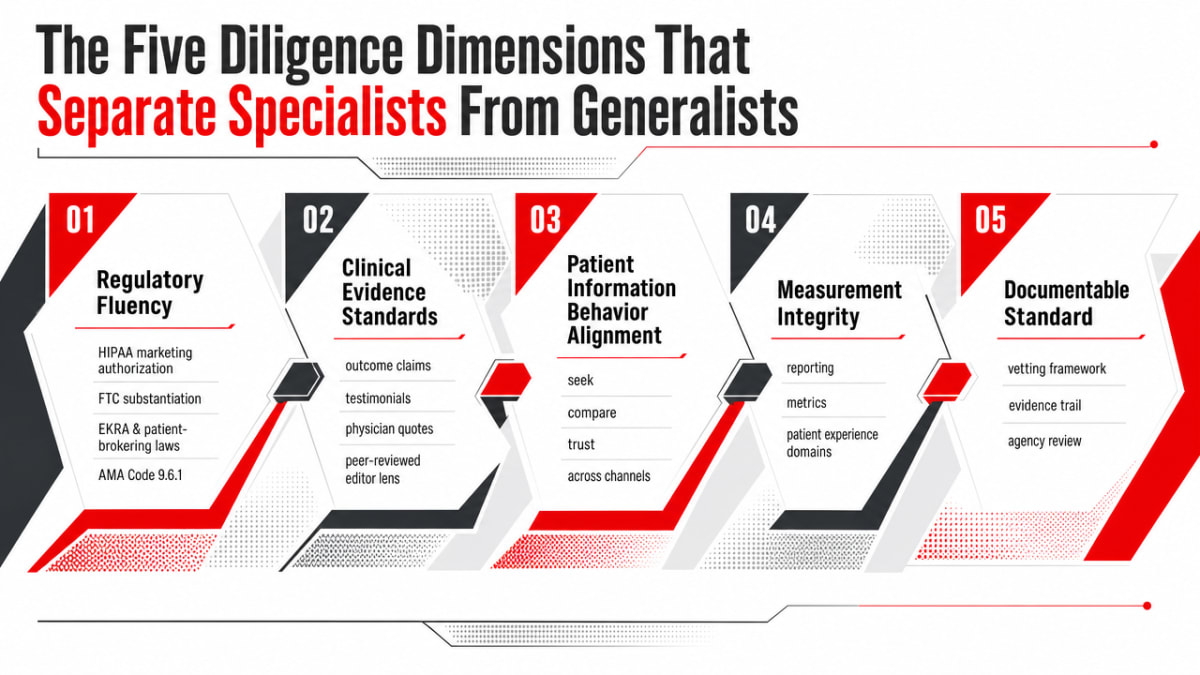
The Five Diligence Dimensions That Separate Specialists From Generalists
A robust vetting process for healthcare content agencies involves five key dimensions, each linked to a documentable standard:
- Regulatory fluency, assessing an agency’s understanding of HIPAA marketing authorization 4, FTC substantiation 5, EKRA and patient-brokering laws 16, and AMA Code 9.6.1 9.
- Clinical evidence standards, evaluating how sample content handles outcome claims, testimonials, and physician quotes, similar to a peer-reviewed editor 3, 5.
- Patient information behavior alignment, ensuring content programs match how patients seek, compare, and trust health information across various channels 1, 10.
- Measurement integrity, which requires reporting on metrics connected to actual patient experience domains 11, rather than superficial traffic data.
- Referral-economics legality, scrutinizing the agency’s pricing models and lead sourcing practices 16.
Dimension One: Regulatory Fluency Across HIPAA, FTC, EKRA, and AMA
HIPAA Marketing Authorization and the PHI Boundary in Digital Channels
The HIPAA Privacy Rule narrowly defines marketing, generally requiring written patient authorization for using or disclosing protected health information (PHI) for marketing purposes, with limited exceptions 4. This has significant implications for common digital marketing tactics.
Tracking mechanisms like pixels on confirmation pages, conversion events linked to specific diagnoses, retargeting audiences built from condition-specific URLs, and lookalike modeling using patient lists can all involve PHI under HHS interpretations 4. An agency must clearly explain, in writing, how it separates marketing analytics from PHI, how its tracking integrates with authenticated patient portals, and which vendors are covered by a Business Associate Agreement (BAA). An agency unable to do so is not suitable for running paid acquisition for a treatment center.
A thorough diligence process should ask the agency to categorize every audience signal it uses into “clearly non-PHI,” “conditional on authorization,” or “prohibited without authorization,” directly referencing HHS marketing guidance 4. Vague assurances of “HIPAA-awareness” are insufficient for regulatory or procurement review.
FTC Substantiation: The Competent and Reliable Scientific Evidence Standard
The FTC mandates that health-related claims be truthful, non-misleading, and supported by competent and reliable scientific evidence, with stronger efficacy claims often requiring well-controlled human clinical testing 5. This standard applies to various content forms, including:
- Landing page copy about recovery rates
- Blog content on modality effectiveness
- Paid ad headlines on outcomes
- Testimonials presented as representative results
An agency proficient in this standard treats outcome language as a sourced assertion, not merely a creative choice. It will consult the clinical team for underlying studies, population data, effect sizes, and limitations before using terms like “proven” or “clinically shown.” It also incorporates disclosure language for testimonials when the described experience is not typical and documents the substantiation file alongside the creative brief 5.
A practical diligence test involves providing the agency with three outcome claims from a competitor’s website and asking them to identify which would pass an FTC review, which would require disclosure, and which would need to be removed. An agency that can perform this exercise, citing the substantiation standard, demonstrates expertise in regulated healthcare content.
EKRA, Patient Brokering, and the Compensation Models That Disqualify an Agency
The Eliminating Kickbacks in Recovery Act (EKRA) and various state patient-brokering statutes criminalize exchanging remuneration for referrals to substance use disorder (SUD) treatment facilities, recovery homes, and clinical laboratories 16. This applies regardless of whether the referral source is a sober-living operator, interventionist, call center, or marketing agency. Compensation structures tied to patient volume are a central enforcement risk.
Therefore, an agency’s pricing model is a primary screening criterion. Per-admission fees, per-VOB bonuses, per-qualified-call commissions, and percentage-of-revenue arrangements all create EKRA exposure when they steer patients to a specific facility 16. Conversely, flat retainers, fixed deliverable fees, and hourly engagements for content production, SEO, and media management generally do not raise the same concerns. An agency proposing a per-admission price for an addiction treatment client should be immediately disqualified.
Diligence requires documentary evidence: request the agency’s standard master service agreement, rate card, and any performance-based addenda. Look for language linking compensation to admissions, intakes, or patient outcomes. Also, cross-reference with the agency’s lead generation practices, including lead origin, qualification methods, and whether any third party in the chain is paid per referral 16.
AMA Code 9.6.1 and the No-Unjustified-Expectations Standard
AMA Code of Medical Ethics Opinion 9.6.1 permits physician advertising but prohibits false, deceptive, or misleading content, specifically warning against unsubstantiated claims, sensationalism, and creating unjustified expectations about treatment 9. The broader Code emphasizes preserving patient trust and public confidence in medicine 8.
For treatment center marketing, this standard impacts the imagery and language used. Content featuring beach sunsets with success rates, before-and-after recovery framing, or emotional testimonials without context can approach the “unjustified expectations” threshold 9. A compliant agency will challenge creative briefs that promise certainty, replace outcome guarantees with realistic descriptions of the care process, and treat physician quotes as clinical statements rather than marketing copy 3, 9.
Ask shortlisted agencies to describe how Opinion 9.6.1 influenced a specific creative decision in a recent campaign. The ability to provide concrete examples demonstrates genuine application of the standard.
Dimension Two: Clinical Evidence Standards in Sample Content Review
While regulatory fluency prevents legal issues, clinical evidence standards ensure content quality. The vetting question here shifts from “is this defensible” to “is this clinically accurate,” as judged by a clinical director. This is revealed in how an agency handles sample work.
Review three pieces from an agency’s portfolio: a long-form article on a modality, a service-line landing page, and a social media post with a patient story. Evaluate them as a peer reviewer would. For instance, does the modality article cite primary literature, or does it rely on other marketing pages? Are effect sizes and patient populations accurately described, or are narrow trial findings generalized 5? Does the landing page present the care pathway as a regulated clinical process, or merely a sales funnel 3?
Patient stories require particular attention. Medical advertising ethics caution against content that creates unjustified expectations or exploits vulnerable individuals, a category that addiction treatment audiences fall into 3. A competent agency presents recovery narratives with appropriate context, timeframes, and acknowledgment of outcome variability, documenting consent and substantiation for each asset. Agencies should also be able to identify the clinician or clinical reviewer who approved each piece, aligning with McKinsey’s concept of medically validated content built on clinical authority 2.
The key signal is process. Request to see the agency’s editorial workflow, substantiation file template, and the names and credentials of clinical reviewers. Agencies that readily provide these artifacts demonstrate adherence to evidence-grade standards.
Dimension Three: Patient Information Behavior and Multi-Channel Defensibility
Pew Research Center’s 2026 survey on health information found that 73% of Americans use multiple sources for health information, with high trust in clinicians and major health organizations, and lower trust in social media and general internet sources 10. This establishes a baseline for how content programs must be constructed.
Patients or family members researching treatments like residential care or telebehavioral programs rarely convert on the first piece of content they encounter. A systematic review of online health information-seeking confirms this multi-channel behavior, influenced by age, education, and health literacy, with consumers triangulating information across search results, organizational websites, social platforms, and clinician discussions before making decisions 1. An agency proposing a single-channel SEO program addresses only a fraction of the actual decision path.
This has direct implications for vetting. Ask each shortlisted agency to audit how their existing treatment-center clients appear across channels identified by Pew data: organic search, owned content, third-party health publishers, social platforms, and clinician-facing referral content. Look for evidence that the agency tracks brand presence and message consistency across these surfaces, not just keyword rankings. The strategic standard to test against is McKinsey’s framework of clinically validated, contextually relevant content designed to engage consumers across multiple touchpoints 2.
The diligence signal is whether the agency designs for information triangulation. Content must remain accurate and consistent when a prospect moves from a service-line page to a third-party recovery publication, then sees a paid social ad, and finally consults a primary care physician. Agencies that build single-asset funnels optimized for one conversion event often fail this test in practice, even if campaign metrics appear acceptable.
Key Metrics for Selecting a Healthcare Content Marketing Agency
Leverage research-driven content strategies that are proven to increase qualified admissions calls and build lasting brand trust in the behavioral health sector.
See Data-Driven ResultsDimension Four: Measurement Integrity Against Patient-Experience Reality
Most agency reports focus on metrics like sessions, rankings, impressions, and cost per lead, which describe the marketing funnel. However, these metrics often fail to indicate whether patients received care consistent with content promises, highlighting a critical gap in healthcare measurement integrity.
AHRQ’s Consumer Assessment of Healthcare Providers and Systems (CAHPS) program measures patient experience across domains such as communication quality and information clarity 11. These domains serve as a reality check for marketing claims. If a landing page promises responsive admissions support, but CAHPS-style feedback reveals long wait times for return calls, the marketing program is creating a measurable promise gap. An agency demonstrating measurement integrity will report on the alignment between acquisition metrics and patient-experience signals, even when the findings are unfavorable.
The diligence request is structural: ask for the agency’s reporting template. Look for three key connections:
- Acquisition metrics tied to qualified admissions (not just form fills)
- Reconciliation of messaging with intake and post-admission feedback
- A documented process for revising or removing content when actual experience deviates from advertised experience 11, 3
Agencies unable to describe how they close this loop are reporting on traffic, not on the program a CMO is ultimately accountable for.
Dimension Five: Sector-Specific Accuracy for SUD, OTP, and Telebehavioral Content
Beyond general healthcare regulations, addiction treatment marketing operates within a stricter set of federal frameworks. SAMHSA compiles statutes, regulations, and guidelines for SUD treatment, including rules for opioid treatment programs (OTPs) and medication-assisted treatment 12. These rules dictate what services can be promised and how they are described in patient-facing content. An agency unfamiliar with relevant SAMHSA frameworks during a discovery call is likely unprepared to create clinically defensible copy.
The OTP case provides a clear test. SAMHSA’s OTP guidance outlines requirements for patient-centered care planning, assessment, and admission processes 13. A landing page that promises same-day intake or an ad implying immediate access to methadone or buprenorphine without detailing regulated assessment and admission steps misrepresents a federally regulated process. Ask the agency to review an existing OTP page and identify where the copy deviates from the SAMHSA-defined care pathway. Specific edits demonstrate sector fluency, unlike vague reassurances.
Telebehavioral health content also requires specialized review. The SGIM telehealth position statement details ethical and practical considerations in virtual care, including transparency about limitations, privacy, and access 18. Agencies creating content for virtual IOPs, telehealth MAT bridges, or remote counseling should integrate these limitations directly into the content, rather than burying them in disclaimers. A capable partner can explain how they address modality boundaries, state licensure disclosure, and crisis-escalation language in telebehavioral assets, citing the SGIM position statement as their guiding standard 18.
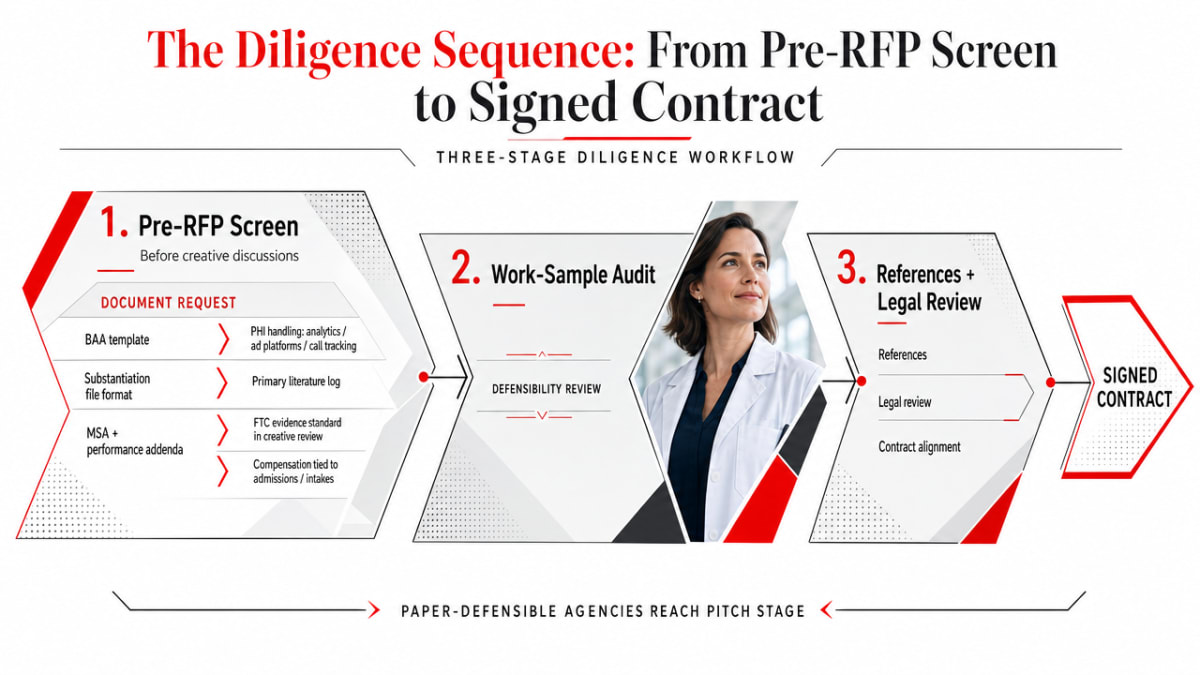
The Diligence Sequence: From Pre-RFP Screen to Signed Contract
Pre-RFP Screen and Document Request
The pre-RFP screen occurs before any creative discussions, aiming to eliminate agencies unable to provide the necessary documentation for a regulated content program. This ensures that only agencies defensible on paper reach the pitch stage.
Three key documents are crucial:
- Request the agency’s current Business Associate Agreement (BAA) template and inquire how it addresses PHI handling across analytics, ad platforms, and call tracking vendors 4.
- Ask for the substantiation file format used for outcome claims, including how primary literature is logged and how the FTC’s competent and reliable scientific evidence standard is applied to creative review 5.
- Request the master service agreement and any performance-based addenda, checking for compensation tied to admissions, intakes, or qualified calls 16.
Agencies that provide these artifacts within a week should be shortlisted. Those that promise to draft them post-contract should be excluded.
Work-Sample Audit Against CDC Plain Language and AMA Standards
Many agencies that pass the document request stage fail the work-sample audit. Select six assets from each shortlisted agency: two service-line landing pages, two long-form articles, a paid social ad, and an email nurture sequence. Score each against its specific governing standard, not a generic content quality rubric.
- Landing pages are evaluated against HIPAA marketing boundaries, particularly how tracking and form data interact with PHI 4.
- Outcome claims and testimonials are subjected to the FTC substantiation test, requiring a documented evidence trail 5.
- Physician quotes and messaging implying treatment certainty are assessed against AMA Code 9.6.1, focusing on avoiding unjustified expectations and sensationalism 9.
- Readability across all six assets is scored using the CDC plain language checklist: audience-first framing, most important information at the top, everyday language, and clear organization 7.
References, Legal Review, and Contract Terms
Reference calls in healthcare marketing should function as diligence interviews. Speak with at least two current clients and one former client. Ask if the agency ever challenged a creative brief on regulatory grounds, how it handled FTC-style substantiation questions, and whether any compensation arrangements were renegotiated towards per-admission terms during the engagement 5, 16.
Before signing, route the proposed contract through healthcare counsel. Counsel should confirm BAA coverage for every vendor in the tracking and analytics stack 4, identify any performance addenda that could trigger EKRA concerns 16, and verify that creative approval workflows grant clinical reviewers genuine veto authority, not just courtesy sign-off 3. The contract resulting from this review is designed to withstand future enforcement scrutiny.
If You Manage Multiple Facilities: Centralized vs. Per-Location Content Economics
This section is relevant for CMOs overseeing multiple facilities, PE-backed platforms, and regional behavioral health groups. Single-site operators may skip ahead.
Portfolio operators face a unique agency-vetting question: how much of the content program can be scaled as shared infrastructure versus what needs to be rebuilt for each facility. This impacts both the scope of work and the regulatory exposure, as each location has distinct clinical staff, service offerings, and state-level rules under SAMHSA frameworks 12.
As no specific cost benchmarks for treatment-center marketing retainers are available, the table below uses qualitative tiers and variables.
| Cost Driver | Centralized Model | Per-Location Model |
|---|---|---|
| Editorial & clinical review | Shared, fixed | Scales with facility count |
| Service-line landing pages | Templated, location variables | Built per site |
| GBP & local citation maintenance | Not applicable | Per facility, recurring |
| Call tracking & BAA coverage | One vendor stack | Per-line provisioning 4 |
Ask shortlisted agencies to clarify which line items they consider fixed versus variable, and require BAA coverage for every per-location tracking number before contract signing 4.

Frequently Asked Questions
What disqualifies a content marketing agency from working with an addiction treatment center?
An agency is disqualified if its compensation model is tied to admissions, intakes, or qualified calls, as this falls under EKRA and state patient-brokering enforcement 16. Additionally, an inability to provide a Business Associate Agreement, a substantiation file template, or a written explanation of how PHI is isolated from ad platforms and tracking pixels is a disqualifier 4, 5.
How should an agency handle protected health information in digital advertising and retargeting?
The HIPAA Privacy Rule generally requires written patient authorization for PHI use in marketing 4. An agency should categorize all audience signals, pixels, and retargeting lists as non-PHI, conditional, or prohibited. Covered vendors must be routed through a BAA, and tracking should be kept off authenticated portal pages and condition-specific conversion events 4.
What evidence standard should outcome claims and patient testimonials meet?
The FTC requires health claims to be truthful, non-misleading, and supported by competent and reliable scientific evidence, often requiring well-controlled human clinical testing for strong efficacy claims 5. Testimonials for non-typical results need clear disclosure, and supporting literature should be documented in a substantiation file for each creative asset 5. Promotional content must also avoid creating unjustified expectations 3.
Are per-lead or per-admission compensation models legal for SUD marketing agencies?
EKRA and state patient-brokering statutes criminalize remuneration for referrals to SUD treatment facilities, regardless of the referring party 16. Per-admission fees, per-VOB bonuses, and per-qualified-call commissions are within this enforcement zone. Flat retainers and fixed deliverable fees do not pose the same risk 16.
What documents should a CMO request before signing with a healthcare content marketing agency?
Before the pitch stage concludes, a CMO should request four key documents: the Business Associate Agreement template covering analytics, ad, and call-tracking vendors 4; the substantiation file format for outcome claims under FTC standards 5; the master service agreement and any performance addenda, checked for admission-linked compensation 16; and the editorial workflow detailing clinical reviewer names, credentials, and veto authority 3.
How do you evaluate an agency’s work samples for clinical accuracy and readability?
Each artifact should be scored against its specific governing standard. Landing pages are reviewed against HIPAA marketing boundaries 4, outcome claims and testimonials against FTC substantiation 5, physician-involved messaging against AMA Code 9.6.1 and the no-unjustified-expectations rule 9. Readability across all samples is assessed using the CDC plain language checklist, focusing on audience-first framing, clear organization, and everyday language 7.
References
- Online Health Information Seeking Behavior: A Systematic Review. https://pmc.ncbi.nlm.nih.gov/articles/PMC8701665/
- Health media: How consumer content informs the future of healthcare. https://www.mckinsey.com/industries/healthcare/our-insights/health-media-how-consumer-content-informs-the-future-of-healthcare
- Ethical issues in advertising and promotion of medical units. https://pmc.ncbi.nlm.nih.gov/articles/PMC5711284/
- Marketing | HHS.gov (HIPAA Privacy Rule Guidance). https://www.hhs.gov/hipaa/for-professionals/privacy/guidance/marketing/index.html
- Health Products Compliance Guidance. https://www.ftc.gov/business-guidance/resources/health-products-compliance-guidance
- Patient engagement and the design of digital health. https://pmc.ncbi.nlm.nih.gov/articles/PMC4674428/
- Plain Language Materials & Resources | Health Literacy. https://www.cdc.gov/health-literacy/php/develop-materials/plain-language.html
- The Code of Medical Ethics of the American Medical Association. https://pmc.ncbi.nlm.nih.gov/articles/PMC3399321/
- 9.6.1 Advertising & Publicity (AMA Code of Medical Ethics). https://policysearch.ama-assn.org/policyfinder/detail/Advertising%20and%20publicity?uri=%2FAMADoc%2FEthics.xml-E-9.6.1.xml
- Where Do Americans Get Health Information, and What Do They Trust?. https://www.pewresearch.org/science/2026/04/07/where-do-americans-get-health-information-and-what-do-they-trust/
- About the CAHPS Program and Surveys. https://www.ahrq.gov/cahps/about-cahps/index.html
- Substance Use Disorders: Statutes, Regulations, and Guidelines. https://www.samhsa.gov/substance-use/treatment/statutes-regulations-guidelines
- Become an Opioid Treatment Program (OTP). https://www.samhsa.gov/substance-use/treatment/opioid-treatment-program/become-otp
- Medicare Marketing Guidelines. https://www.cms.gov/medicare/health-drug-plans/managed-care-marketing/medicare-guidelines
- Medicare Communications and Marketing Guidelines (MCMG). https://www.cms.gov/files/document/medicare-communications-marketing-guidelines-2-9-2022.pdf
- What Is Patient Brokering?. https://nccriminallaw.sog.unc.edu/2024/10/07/what-is-patient-brokering/
- Patient engagement strategies in digital health interventions for cancer survivors: a scoping review. https://pmc.ncbi.nlm.nih.gov/articles/PMC10124932/
- Telehealth Policy, Practice, and Education: a Position Statement of the Society of General Internal Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC12124549/