Key Takeaways
- Vendor selection should run as a three-domain audit covering regulatory fluency, behavioral-health communication craft, and evidence discipline rather than a generic capability checklist that fails to distinguish specialized partners.
- A competent partner operates inside AMA Opinion 9.6.1 and can produce an FTC-aligned substantiation file documenting express claims, implied messages, scientific support, study limitations, and review dates 3.
- Behavioral-health craft means person-first language audits using NIDA’s Words Matter standard plus teach-back checkpoints in intake scripts, because stigmatizing terminology measurably suppresses treatment seeking 4, 5.
- Evidence discipline requires attribution that connects spend to qualified calls, VOB completion, and admissions, with CAHPS-aligned experience signals substantiating any compassion or quality claim 11.
- Disqualifying signals include unsourced success rates, outdated stigmatizing terminology, OTP pages still gating on the pre-2024 one-year addiction threshold, and ‘national helpline’ framing that misrepresents SAMHSA infrastructure 16, 17.
- Portfolio operators carry replicated risk across every license, so centralized version control of creative, claims, and intake scripts becomes a weighted requirement rather than an optional coordination feature 15.
- Test finalists with a working session: ask them to produce a substantiation file, redline copy against person-first standards, and rewrite paid search headlines to match 2024-compliant OTP admission language.
The Three Tests Most CMOs Underweight
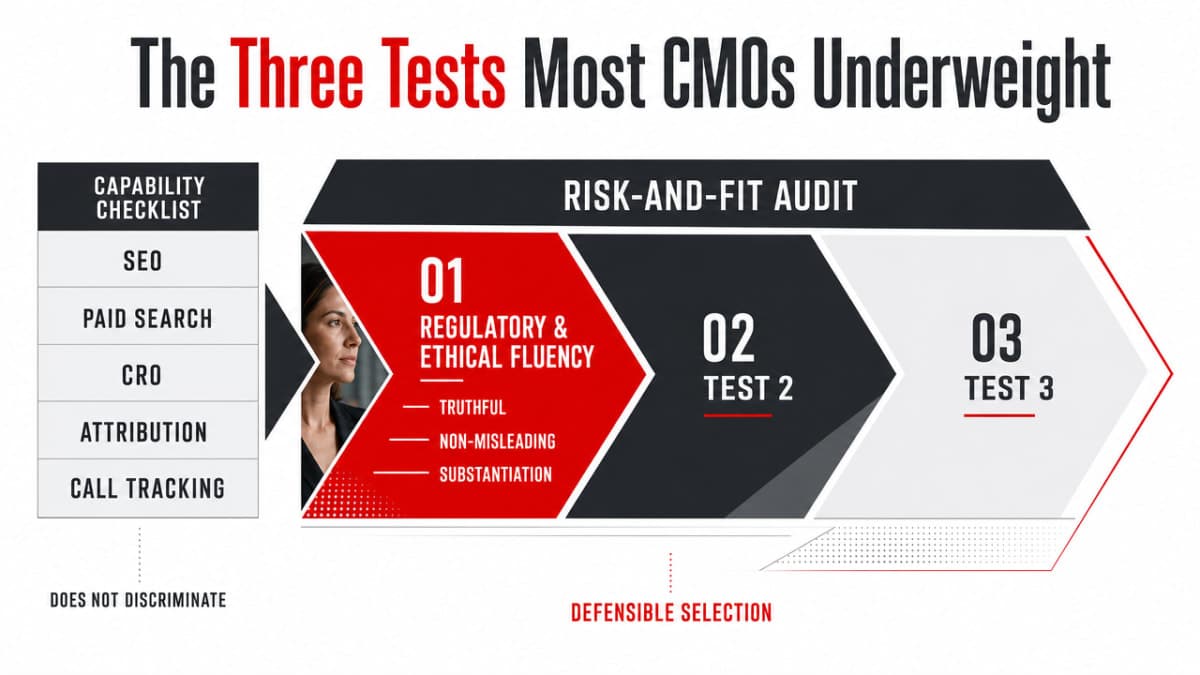
Most vendor-vetting checklists circulating among treatment center marketing leaders read like capability inventories: SEO, paid search, CRO, attribution modeling, call tracking. Every serious agency claims all of it. The checklist, in other words, does not discriminate. It tells a CMO almost nothing about whether the partner across the table can actually move admissions in substance use disorder and behavioral health without quietly creating regulatory exposure or eroding prospect trust.
A more defensible frame treats vendor selection as a risk-and-fit audit organized around three tests:
- The first is regulatory and ethical fluency: does the partner operate inside the AMA’s standard that promotional communications be truthful, non-misleading, and free of unjustified expectations 2, and can they document substantiation for any health-related claim under the FTC’s compliance framework 3?
- The second is behavioral-health communication craft: does the creative, the landing page, and the call script reflect person-first language standards 5 and health-literate spoken communication 6?
- The third is evidence discipline: does the partner tie spend to measurable patient-experience and conversion outcomes rather than rhetoric-heavy dashboards 8?
A vendor who fails any one of the three will either invite enforcement risk or undermine the trust signals that convert calls into admissions. The remainder of this article turns each test into a working scorecard.
Domain One: Regulatory and Ethical Fluency
The AMA 9.6.1 Standard a Competent Partner Operates Inside
The AMA’s Opinion 9.6.1 is not a marketing constraint to work around. It is the operating standard a healthcare marketing expert should be able to recite from memory. The policy frames physician advertising restrictions narrowly: they exist to prevent deception, not to suppress promotion 2. That distinction matters for a CMO building a vendor scorecard, because it shifts the question from “what can we say?” to “what can we substantiate, present in context, and defend if challenged?”
The Code of Medical Ethics organizes its guidance on physician communications across opinions covering confidentiality, advertising, and media relations, treating public-facing speech as an extension of the clinical relationship rather than a separate commercial activity 1. A partner who treats admissions creative as ordinary direct-response work — testimonials stripped of context, before-and-after framing, vague recovery promises — is working from a different rulebook than the one clinical leadership operates inside.
The vetting move is straightforward. Ask the partner to walk through a recent campaign and identify three things: the material information disclosed to prospective patients, the specific claims that could create unjustified expectations, and the documentation trail for both. A competent partner produces this without hesitation. A generic healthcare marketer treats the question as a compliance interruption and redirects to performance metrics.
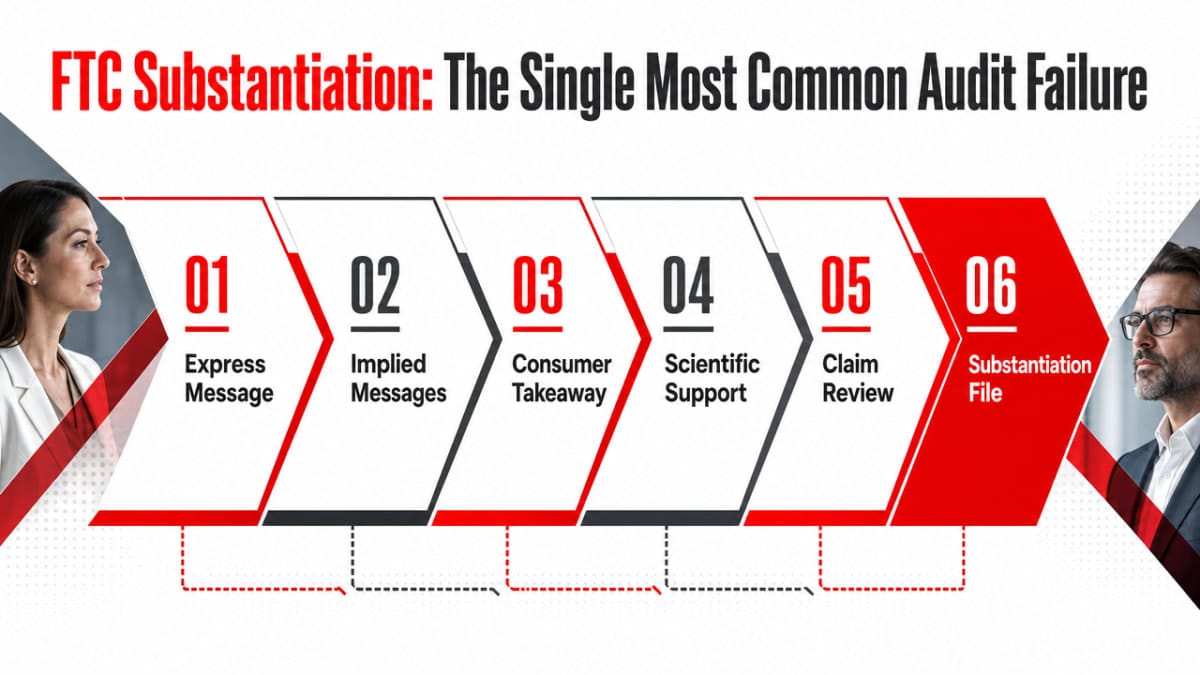
FTC Substantiation: The Single Most Common Audit Failure
Most admissions campaigns fail their first serious legal review at the same point: an outcome claim, a success rate, or an implied benefit that no one on the marketing side can defend with a paper trail. The FTC’s Health Products Compliance Guidance, updated in December 2022, is explicit about what defense looks like. Marketers must “consider what express and implied messages consumers are likely to take” from a piece of creative and “carefully review the support for each claim” to confirm it is scientifically sound 3.
That standard collapses into a working artifact: a substantiation file. A competent partner should be able to produce one on demand for any health-related claim running in market. The file documents:
- the express message,
- the implied messages a reasonable consumer would take,
- the scientific support relied on,
- the study design and population,
- the limitations of that evidence, and
- the date of the most recent review 3.
A vendor who has never assembled one — or who treats the request as excessive — is not a behavioral health partner. They are a lead-gen vendor working in a regulated space without the right paperwork.
Implied messages are where most agencies stumble. A landing page headline reading “Get your life back” is not a literal outcome claim, but the FTC’s analysis turns on what consumers reasonably take from the message, not what the marketer intended 3. A photograph of a smiling family next to language about “proven recovery” carries a substantiation burden even when no percentage appears on the page. Vetting should include a walkthrough of how the partner audits implied claims in active creative, not just the headline assertions a junior reviewer would flag.
Regulatory Currency: The 42 CFR Part 8 Test
Regulatory fluency is not a static credential. A partner who passed a 2020 compliance check may be working from a rulebook that no longer applies. The cleanest currency test available to a CMO right now is SAMHSA’s 42 CFR Part 8 final rule, updated in February 2024 and effective October 2024, which restructured admission criteria and operational flexibility for opioid treatment programs 17.
The substantive changes matter for admissions messaging. Admission requirements no longer rely on the prior one-year opioid addiction threshold or documentation of multiple failed detox attempts, and the rule expands evidence-based delivery models including telehealth pathways 17. The proposal phase, summarized by the American Hospital Association in late 2022, signaled the direction of travel a year before the rule landed 12. A partner tracking the sector should have adjusted OTP client landing pages, paid search copy, and intake scripts to reflect the new eligibility language well before the effective date.
Ask the partner directly: how did the 2024 OTP rule change the campaigns they run for opioid treatment clients? A current partner answers with specifics — copy updates, eligibility FAQ revisions, telehealth-pathway landing pages. A partner who needs to look it up, or who conflates 42 CFR Part 8 with Part 2 confidentiality rules, is not operating with the regulatory currency a treatment center license depends on.
Domain Two: Behavioral-Health Communication Craft
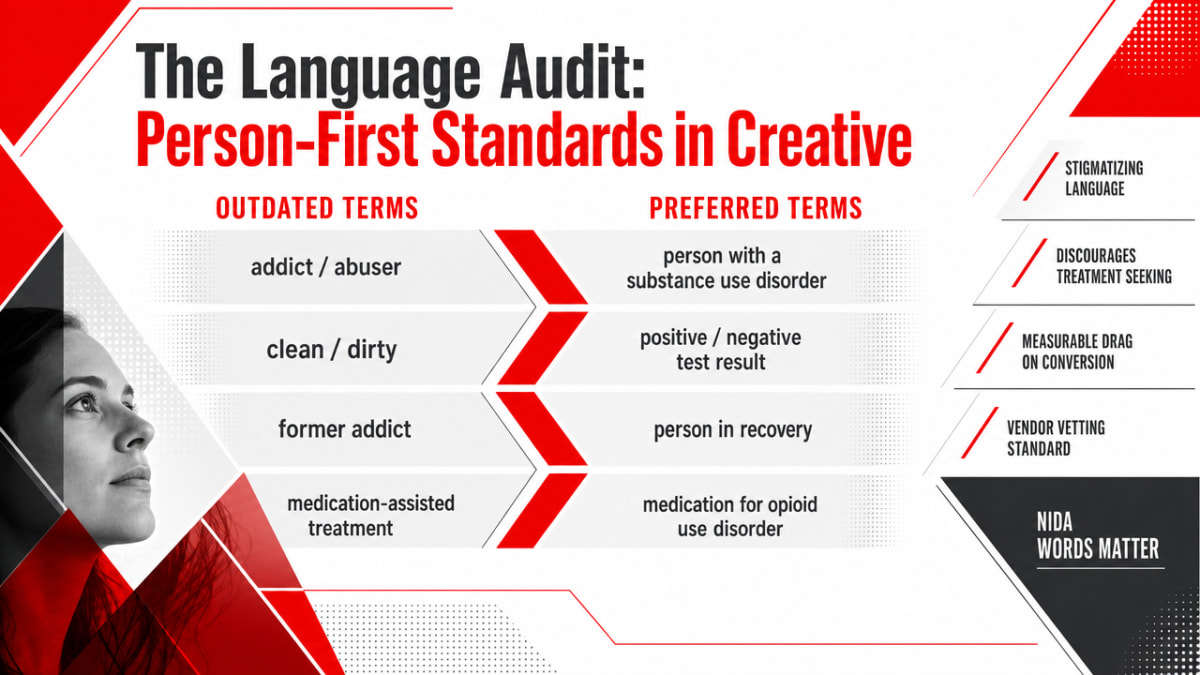
The Language Audit: Person-First Standards in Creative
Stigma toward people with substance use disorders persists across health professionals, driven by moral models of SUD and gaps in addiction-specific training, and stigmatizing language in public communications discourages treatment seeking in the exact population an admissions campaign is trying to reach 4. The implication for vendor vetting is direct: creative that uses outdated terminology is not a stylistic preference. It is a measurable drag on conversion among prospects already weighing whether to make the call.
NIDA’s Words Matter guidance translates the research into a working terminology standard:
- “Person with a substance use disorder” replaces “addict” or “abuser.”
- “Positive” or “negative test result” replaces “clean” or “dirty.”
- “Person in recovery” replaces “former addict.”
- “Medication for opioid use disorder” replaces “substitution” or “replacement therapy.”
NIDA frames the standard plainly: feeling stigmatized reduces willingness to seek treatment, and communicators should take all steps necessary to reduce the potential for stigma and negative bias 5.
A competent partner conducts a language audit as a standing creative-review step, not a one-time cleanup. The audit covers:
- paid search headlines and descriptions,
- landing page H1s and body copy,
- image alt text,
- retargeting ad variants,
- call-script openings,
- voicemail templates, and
- the form-confirmation and email-nurture sequences that follow a submission.
It also extends to family-facing pages, where “loved one struggling with addiction” requires the same scrutiny as patient-facing copy.
The vetting move: ask the partner to produce a redlined sample of their own prior creative against the NIDA standard. A partner who has done the work hands over a marked-up artifact. A partner who has not done the work argues that their copywriters “already know” — which is the response the underlying stigma research predicts and warns against 4.
The Marketing-to-Admissions Handoff: Teach-Back at the Call Stage
Most vendor pitches end at the form fill. The admissions pipeline does not. The conversion that matters — the qualified call that becomes a VOB conversation and then an admission — runs through a spoken exchange where the prospect or family member is often distressed, time-pressured, and parsing insurance language they have never encountered. A marketing partner who cannot speak to call-stage communication craft is handing the CMO a lead and walking away from the place where the lead is actually won or lost.
AHRQ’s spoken-communication toolkit gives the standard. The agency recommends a universal-precautions approach to health literacy, treating every patient interaction as if comprehension may be limited, and using teach-back — asking the caller to repeat back what they heard in their own words — to confirm understanding before moving forward 6. Applied to admissions intake, that means the VOB conversation does not end when the benefits are read aloud. It ends when the caller can restate, in plain language, what their plan covers, what the next step is, and when they will hear back.
A competent partner shows up to the vetting conversation with artifacts:
- an intake script with teach-back checkpoints at benefits explanation, level-of-care recommendation, and next-step confirmation;
- a plain-language glossary substituting “the portion you pay” for “coinsurance”; and
- a QA rubric scoring calls on comprehension confirmation, not just call duration or disposition.
Centralized review of these artifacts across marketing, clinical intake, and compliance reflects the coordination AHRQ recommends for any health-services outreach program 15.
Crisis Messaging and the Public Referral Line
One bright line should never be crossed. SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service available in English and Spanish 16. It is public infrastructure. Paid search creative, landing pages, and chat widgets that mimic the helpline’s framing, suggest a public-resource affiliation that does not exist, or position a private intake line as the federal referral service misrepresent the public safety role of that infrastructure.
The vetting test is concrete. Review the partner’s active paid search ad copy for any branded or implied use of “national,” “helpline,” “hotline,” or government-style language without clear sponsor identification. Review crisis-keyword bidding strategy: does the partner bid on suicide and overdose terms, and if so, what is the routing protocol when the caller’s need exceeds the center’s level of care? A partner without a documented answer is not ready for crisis-adjacent traffic.
Domain Three: Evidence Discipline
Against Vanity Metrics and Tech Rhetoric
The reporting layer is where most agency relationships go quietly wrong. Impressions climb, click-through rates look healthy, the monthly deck is full of green arrows, and admissions volume sits flat. A partner with evidence discipline does not lead with traffic. They lead with the chain that connects spend to a qualified call, a completed VOB, and an admission — and they are explicit about where the chain breaks.
The peer-reviewed review of digital marketing in healthcare names the trade-off directly: post-pandemic acceleration has expanded reach, but campaigns must balance growth ambitions with ethical communication, data protection, and accurate health information 7. Volume that comes from misinformation-adjacent creative or aggressive crisis-keyword bidding is not progress. It is liability with better attribution.
The tech-rhetoric problem is adjacent and worth naming. Vendors increasingly pitch AI personalization, predictive lead scoring, and conversational agents as admissions accelerants. The consumer-engagement-in-health-IT analysis pushes back: optimistic narratives about engagement technology routinely outrun the empirical evidence, and serious work requires better data on whether these tools actually move national health goals 8. A competent partner can describe what their AI stack does, what it has been measured against, and where it has failed. A partner who answers “AI” to every question about attribution, personalization, or conversion is selling rhetoric.
CAHPS-Aligned Experience Signals as Substantiation
Experience claims are the second-most-common audit failure after outcome claims. “Compassionate care,” “family-centered approach,” “industry-leading patient experience” — these appear on nearly every treatment center website, and almost none of them are tied to a measurement instrument the FTC would recognize as substantiation.
AHRQ’s CAHPS Outpatient Mental Health Survey collects standardized data on adult experiences with mental health and substance use disorder services across settings, covering access, communication, and coordination 11. The broader CAHPS literature documents how patient-experience survey data supports patient-centered improvement and quality initiatives when administered systematically, as NCQA recommends for medical-home transformation 10. A partner who treats experience as a creative talking point rather than a measured construct cannot defend an experience claim under scrutiny.
The vetting move is to ask the partner how they would substantiate the experience language on a client’s existing landing page. A competent answer references CAHPS-aligned items the center either already collects or could collect, names the specific composites (access, communication, coordination) the claim maps to, and proposes a review cadence. A weak answer offers more testimonials. Testimonials are not substantiation under the FTC framework; standardized survey data is.
What to Inspect Inside a Case Study
Case studies are the artifact every agency offers and almost no one inspects properly. The standard reading — admissions up, cost per lead down, a quote from the COO — answers none of the questions a CMO building a defensible scorecard actually needs answered. Inspection should run through the three domains the rest of this article has built out.
On regulatory and ethical fluency, the case study should reference the substantiation file behind any outcome or experience figure cited, and the creative samples shown should be defensible under the AMA standard that promotional communications be truthful, non-misleading, and free of unjustified expectations 2. If a success rate appears in the deck with no methodology footnote, the partner has just demonstrated the failure mode.
On behavioral-health communication craft, the case study should include before-and-after creative showing a language audit applied, and intake-script excerpts or QA rubrics demonstrating teach-back checkpoints at the call stage. On evidence discipline, the case study should show the attribution model used, the patient-experience signals tracked alongside conversion, and at least one honest account of what did not work and why.
A case study without these elements is a marketing artifact about marketing. A case study with them is a working document a CMO can defend to clinical leadership, compliance, and the CFO in the same meeting.
Key Metrics for Evaluating Healthcare Marketing Expertise
Leverage industry-specific analytics and proven digital strategies to ensure your admissions marketing delivers measurable, compliant results for behavioral health organizations.
Assess Your StrategyDisqualifiers: Signals That Should End the Conversation
Some signals do not warrant a follow-up call. They warrant ending the meeting and reallocating the search budget.
- A success-rate or completion-percentage figure on the agency’s own site or in a case study deck, presented with no methodology footnote, no study population, and no review date. The FTC’s substantiation standard does not bend for marketers operating in behavioral health 3. A vendor who treats their own outcome claims this way will treat a client’s the same.
- Creative samples that use “addict,” “clean,” “abuser,” or “substitution therapy” in current production work. The terminology standard has been public for years, and the underlying stigma research is unambiguous about how language shapes treatment seeking 4. A partner still shipping this copy is not specialized.
- An OTP client landing page or paid search ad that still gates eligibility on a one-year addiction history or repeated failed detox attempts. SAMHSA’s 42 CFR Part 8 final rule removed that gate, and a partner who has not updated client assets is not tracking the rule changes that govern their clients’ licenses 17.
- Paid search creative using “national helpline” framing or government-style language without clear sponsor identification. Misrepresenting public referral infrastructure is a bright line, not a gray area 16.
- An attribution conversation that ends at form fills, with no view into call quality, VOB completion, or admission. A partner who cannot connect spend to admissions is selling traffic, not pipeline 7.
A Note for Portfolio Operators
The calculus shifts for multi-site behavioral health operators. A CMO running a single facility absorbs vendor risk inside one license. A VP of Growth overseeing six, ten, or twenty locations across multiple states is exposing every license to the same creative system, the same intake scripts, and the same substantiation gaps. One non-compliant landing page replicated across a portfolio is not a single-facility problem. It is a portfolio-wide enforcement footprint.
Portfolio operators should weight regulatory and ethical fluency higher than a single-facility scorecard would suggest, and require centralized review of marketing and stakeholder outreach across the brand family — the coordination posture AHRQ recommends for any health-services outreach program 15. Ask the partner how creative, claims, and intake scripts are version-controlled across sites, how a 42 CFR Part 8 update propagates to every OTP location simultaneously 17, and who owns the substantiation file when the same outcome claim runs in three states. A partner without an answer is acceptable risk on one license and unacceptable risk on twenty.
Putting the Scorecard to Work
The three domains do not carry equal weight in every search. A center expanding an OTP line should weight regulatory currency higher; a center repositioning around clinical differentiation should weight communication craft and CAHPS-aligned substantiation higher 11. The scorecard is a tool, not a formula.
Run finalists through one working session before signing. Hand them a current landing page and ask three things:
- produce the substantiation file for the strongest claim on the page 3,
- redline the copy against person-first terminology 5, and
- map two paid search headlines to the admission-criteria language a 2024-compliant OTP page should use 17.
Sixty minutes of artifact-level work tells a CMO more than six weeks of pitch decks.
The partner who treats those three asks as standard practice — not a special request — is the one who can move admissions without quietly creating the exposure that erases the gains.
Frequently Asked Questions
What separates a healthcare marketing expert from one qualified to drive behavioral health admissions?
A general healthcare marketer can run branded search, build a responsive site, and report on click volume 18. A behavioral health admissions partner adds three capabilities: documented adherence to AMA 9.6.1 truthful-advertising standards 2, person-first language standards traceable to NIDA’s Words Matter guidance 5, and an attribution model that ties spend to qualified calls and VOB outcomes, not form fills 7.
What should a substantiation file contain before we approve any outcome or recovery claim in a campaign?
Under the FTC’s Health Products Compliance Guidance, the file should document the express claim, the implied messages a reasonable consumer would take from the creative, the scientific support relied on, the study design and population, the limitations of that evidence, and the date of the most recent review 3. If any element is missing, the claim does not run.
How do we test whether a marketing partner is current on the 2024 SAMHSA 42 CFR Part 8 changes?
Ask how the rule changed their OTP client campaigns. A current partner cites specifics: removal of the one-year opioid addiction admission threshold, elimination of the multiple-failed-detox documentation requirement, and updated landing pages reflecting telehealth pathways 17. A partner who conflates Part 8 with Part 2 confidentiality rules, or who needs to research the answer, is not tracking the regulatory environment their clients operate inside.
What does a language audit look like, and who should perform it?
A language audit redlines active creative against NIDA’s terminology standard, replacing “addict,” “clean,” “abuser,” and “substitution therapy” with person-first equivalents across ads, landing pages, alt text, call scripts, and nurture emails 5. The agency should perform it as a standing creative-review step, with clinical or compliance sign-off, because stigmatizing language measurably reduces willingness to seek treatment among the prospects being targeted 4.
Should a marketing vendor have a role in admissions call handling and VOB conversations?
Yes, at the script and QA level. AHRQ’s spoken-communication guidance recommends a universal-precautions approach to health literacy, using teach-back to confirm a caller understands benefits, level-of-care recommendations, and next steps before the call ends 6. A partner who hands over leads and walks away from call quality is selling traffic. A partner who co-owns the script and QA rubric is selling pipeline.
Which disqualifying signals should end a vendor conversation immediately?
Four end the meeting: outcome figures presented without methodology, population, or review date 3; current creative using “addict,” “clean,” or “substitution therapy” 5; OTP landing pages still gating eligibility on the pre-2024 one-year addiction threshold 17; and paid search copy using “national helpline” framing without clear sponsor identification, which misrepresents SAMHSA’s public referral infrastructure 16. Each is a documented standard, not a preference.
References
- The Code of Medical Ethics of the American Medical Association. https://pmc.ncbi.nlm.nih.gov/articles/PMC3399321/
- 9.6.1 Advertising & Publicity. https://policysearch.ama-assn.org/policyfinder/detail/Advertising%20and%20publicity?uri=%2FAMADoc%2FEthics.xml-E-9.6.1.xml
- Health Products Compliance Guidance. https://www.ftc.gov/business-guidance/resources/health-products-compliance-guidance
- Stigmatization of people with addiction by health professionals. https://pmc.ncbi.nlm.nih.gov/articles/PMC10656222/
- Words Matter: Terms to Use and Avoid When Talking About Addiction. https://nida.nih.gov/nidamed-medical-health-professionals/health-professions-education/words-matter-terms-to-use-avoid-when-talking-about-addiction
- Spoken Communication – Health Literacy Improvement Tools. https://www.ahrq.gov/health-literacy/improve/precautions/guide/spoken.html
- The impact and challenges of digital marketing in the health care industry. https://pmc.ncbi.nlm.nih.gov/articles/PMC9366108/
- Consumer Engagement in Health IT: Distinguishing Rhetoric from Reality. https://pmc.ncbi.nlm.nih.gov/articles/PMC4672873/
- The Future of Public Mental Health: Challenges and Opportunities. https://pmc.ncbi.nlm.nih.gov/articles/PMC10126977/
- Using CAHPS® Patient Experience Data for Patient-Centered Medical Home Transformation. https://pmc.ncbi.nlm.nih.gov/articles/PMC10337703/
- CAHPS Outpatient Mental Health Survey. https://www.ahrq.gov/cahps/surveys-guidance/mental-health/index.html
- SAMHSA rule aims to expand access to opioid treatment programs. https://www.aha.org/news/headline/2022-12-13-samhsa-rule-aims-expand-access-opioid-treatment-programs
- Improving Health Through Health Marketing. https://pmc.ncbi.nlm.nih.gov/articles/PMC1636721/
- Conceptual Model for the Integration of Marketing Strategies and Biomedical Technology in Healthcare. https://pmc.ncbi.nlm.nih.gov/articles/PMC12772582/
- Section 5: Marketing and Stakeholder Outreach. https://www.ahrq.gov/research/publications/pubcomguide/pcguide5.html
- National Helpline for Mental Health, Drug, Alcohol Issues. https://www.samhsa.gov/find-help/helplines/national-helpline
- 42 CFR Part 8 Final Rule: Expanding Access and Flexibility for Opioid Treatment Program Patients. https://www.samhsa.gov/substance-use/treatment/opioid-treatment-program/42-cfr-part-8/for-patients
- What Is Healthcare Marketing? Tips for Branding Your Practice. https://publichealth.tulane.edu/blog/healthcare-marketing/