Key Takeaways
- Treat the homepage as a clinical intake instrument that answers three questions fast: does this facility treat my situation, how do I reach a human, and can I trust them with a disclosure.
- Operationalize NIDA principles through a persistent call element, a level-of-care selector in primary navigation, and visible whole-person content, so visitors arrive at the admissions call already routed 5.
- Language and imagery carry a measurable stigma tax; person-first copy and real clinical photography reduce friction backed by CDC guidance and help-seeking research 4, 3.
- Before February 16, 2026, audit every form, pixel, chat widget, and CRM connection against the updated 42 CFR Part 2 consent and disclosure framework 10.
The homepage as first clinical touchpoint
A treatment center homepage is not a marketing surface. It is the first clinical contact most prospective patients and families ever have with a facility, and its design either supports a care decision or blocks one. Research on online health information seeking finds that users under stress prioritize clarity, credibility, and ease of navigation, and that poor usability and complex language directly impair understanding and decision-making 2. Translated into operator terms: a homepage that buries the call button, hides level-of-care information behind jargon, or leads with stock recovery imagery is losing admissions before the intake team ever picks up the phone.
Treatment center operators already understand the economics of an empty bed. What often goes unexamined is how much of the admissions leak happens in the first ten seconds of a homepage visit, before any tracked event fires. A person in crisis, or a family member acting on their behalf, is scanning for three things: whether this facility treats their situation, how to reach a human, and whether the organization can be trusted with a disclosure that carries legal and social weight. Everything that follows in this guide treats the website as a clinical intake instrument built to answer those three questions faster than the next tab the visitor has open.
Triage architecture: routing visitors to the right level of care
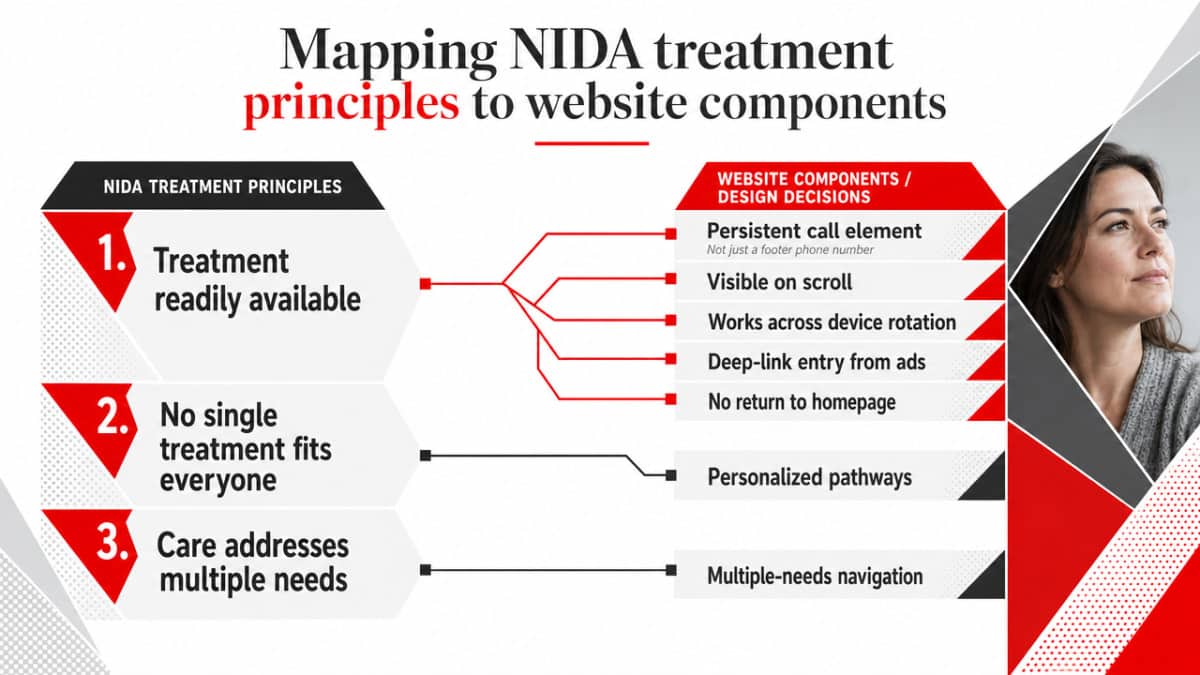
Mapping NIDA treatment principles to website components
The clinical literature already specifies what a good front door to addiction care does. NIDA’s research-based guide is explicit on three points that should shape every primary page on a treatment center site:
- treatment must be readily available,
- no single treatment is appropriate for every individual, and
- effective care attends to multiple needs of the person, not just drug use 5.
Operators rarely dispute the principles. The gap is that most sites do not translate them into design decisions an admissions team can defend.
Readily available, on a website, is not a phone number in the footer. It is a persistent call element that survives scroll, device rotation, and deep-link entry from a paid search ad. A visitor who lands on a blog post about fentanyl withdrawal at 2 a.m. should not have to return to the homepage to find a route to a human. The same principle governs response time on forms and chat: if a tool collects contact information, the site should set the expectation of when a clinician or admissions coordinator responds, because availability that fails on first contact is indistinguishable from no availability at all.
The principle that no single treatment fits everyone is operationalized as a level-of-care selector on the primary navigation 5. Detox, residential, PHP, IOP, outpatient, and MAT each carry different clinical criteria and different admissions workflows. A site that funnels every visitor into a single “Get Help Now” form forces the intake team to do triage work the website should have handled. A site that lets the visitor self-identify the level of care they think they need produces a qualified call with context attached.
Attending to multiple needs translates into visible content on co-occurring disorders, medical comorbidities, family involvement, and aftercare. The Massachusetts person-centered care framework reinforces the same standard: care should be transparent, with knowledge and information shared freely as the individual’s needs change 7. Operators who treat these as separate microsites or buried subpages effectively tell prospective patients that complexity is someone else’s problem. The component map is simple to state and harder to execute: persistent call CTA, level-of-care selector, and co-occurring or whole-person content surfaced from the homepage, each tied to a NIDA principle that an admissions director can defend in a clinical meeting.
Structured assessment pathways and the ASAM intake question
The California SUD intake study compared three approaches to assessment and level-of-care decision-making across county systems, including a standardized ASAM-based model, and found that the structure of intake affects where patients land and whether they stay 1. The operational takeaway for a website is narrower than the study itself: the digital front door cannot replicate a clinician’s ASAM assessment, but it can preserve enough structure that the visitor arrives at the admissions call already routed toward the correct pathway.
Two design decisions follow. First, the site should explain levels of care in language that maps to what an admissions clinician will actually ask. A page that describes residential treatment without naming the clinical indications a coordinator screens for leaves the visitor unprepared and the intake call longer. Second, any pre-screening tool the site offers should be framed honestly. It is a guide to a clinical conversation, not a diagnosis. The California work points to engagement and retention consequences when structured intake is done well 1; the inverse risk is that a flashy self-assessment quiz that overpromises a level-of-care recommendation can erode trust before the call even connects.
The practical configuration most facilities can defend looks like this. Each level-of-care page carries a short, plain-language indication summary, a clear next step that routes to a human, and an honest statement that final placement is determined by clinical assessment. Insurance verification sits adjacent to that pathway rather than gating it, because forcing a payer check before a clinical conversation filters out exactly the visitors most likely to convert. Structured intake on the site is not about replicating ASAM dimensions in a form field. It is about ensuring the admissions team picks up a phone with the visitor already pointed toward the right door.
Language, imagery, and the stigma tax on admissions calls
Stigma is the most underpriced variable on a treatment center website. The CDC frames it plainly: stigma refers to negative attitudes and stereotypes toward people with mental health and substance use conditions, and it can prevent or delay people from seeking care 4. A homepage that uses clinical condescension, recovery-cliché stock photography, or words a person would not say out loud to a friend is taxing every paid click before the call ever connects.
The review evidence on help-seeking sharpens the operator implication. Stigma reduces or delays help-seeking, and message framing is one of the levers that moves it 3. For treatment center operators, that maps to two surfaces the website controls completely: word choice and imagery. Both are cheap to change and rarely audited with the same rigor as page speed or schema markup.
The language swap is concrete:
- “Addict” becomes “person with a substance use disorder.”
- “Clean” becomes “in recovery” or “not currently using.”
- “Substance abuser” becomes “person who uses drugs.”
- Relapse” stays clinical when describing a care episode but is replaced by “return to use” in patient-facing copy.
- “Dirty test” has no place on a website at all.
The CDC guidance is explicit that non-stigmatizing language is one of the few strategies with public health backing for reducing the barrier 4, and the help-seeking literature ties that framing directly to whether people present for care 3. An admissions team that picks up a phone after the visitor has read person-first language across the site is starting the call with less defensiveness on the other end.
Imagery carries the same weight and is more often mishandled. Silhouettes on cliffs, hands gripping bars, and grayscale portraits of despair signal that the facility sees its patients as case studies rather than people. The replacement standard is not aspirational sunsets either. Photography that shows clinicians at work, group settings without dramatized anguish, and real facility interiors does two things at once: it reduces the stigma cue and provides a trust signal about what the visitor would actually walk into. Lived-experience content, framed respectfully, is identified in the CDC guidance as a stigma-reduction strategy 4, which means staff and alumni stories belong on the site as primary content rather than buried testimonial widgets.
Tone is the third surface. Copy that lectures, warns, or moralizes about substance use signals that the organization will do the same in person. Copy that explains what happens on a first call, who answers, what is asked, and what is not asked removes friction the visitor is already carrying. The help-seeking review notes that stigma also causes people to discontinue treatment once started 3, so the same language standards that govern the homepage need to extend to confirmation emails, intake forms, and any automated text the CRM sends after a form submission. A site that gets the homepage right and then sends a “Thank you for reaching out about your addiction” email has undone its own work between two systems the operator owns.
Telehealth access as a primary site element
Telehealth belongs in the primary navigation, not on a tertiary services page. A 2024 meta-analysis of user acceptability for tele-mental health services delivered through online and web-based platforms found generally high acceptance among users, indicating that prospective patients now expect remote care as a legitimate entry point rather than a backup option 8. Treatment center operators who keep virtual IOP, telehealth MAT consultations, or remote counseling buried two clicks deep are filtering out a segment of qualified visitors who would have called if the option had been visible above the fold.
The clinical case for surfacing telehealth is stronger than the acceptability data alone. The VA Evidence Synthesis Program brief reviewing telehealth-delivered mental health treatment found that, for conditions like depression and PTSD, symptom outcomes via videoconferencing or telephone can be similar to in-person care, based on low to moderate strength evidence 9. That evidence base does not cover every SUD presentation, and operators should not overstate it. What it does support is presenting telehealth as a clinically defensible pathway alongside residential and outpatient options, not as a discount tier.
Design implications are specific. The level-of-care selector should include a virtual track wherever the facility offers one, with the same depth of content the in-person pages carry: who delivers care, what platform is used, what insurance covers it, and how the first session is scheduled. A telehealth page that consists of a single paragraph and a generic form signals that the program is an afterthought, which the visitor reads as a clinical signal even when it is just a content gap.
Data-Driven Website Design for Predictable Admissions
Research shows patient-centered website design increases call conversions and lowers acquisition costs for treatment centers. Discover strategies to align digital experience with admissions goals.
Increase Admissions ConsistencyTrust signals and information transparency
Trust on a treatment center website is built before the visitor reads a single testimonial. The online health information seeking review identifies credibility as one of the core factors that shapes whether users act on what they read, alongside clarity and navigability 2. For a person evaluating a facility at 11 p.m. with a family member on the other end of the call, credibility is read off the surface of the site within seconds: is the clinical leadership named, are accreditations visible, does the language sound like a clinician wrote it, and does the page answer questions a coordinator would otherwise have to handle on a call.
The Massachusetts person-centered care framework names the standard the website should meet. Care should be transparent, with knowledge and information shared freely, and guidance should follow the individual’s changing needs 7. Translated into design, that means the site publishes what most operators still hide behind a phone call: who the medical director is and what their credentials are, which licensures and accreditations the facility holds, what a typical day in each program looks like, what the family communication policy is, and what the discharge and aftercare process includes. Operators sometimes worry that publishing program detail invites comparison shopping. The opposite tends to be true on a call-driven site, because the visitors who self-disqualify on a transparency page were never going to convert into a retained admission.
Five trust signals carry disproportionate weight on a treatment center homepage and program pages:
- Named clinical leadership with credentials and photos.
- Accreditation marks from Joint Commission or CARF placed where they are actually seen, not in a footer.
- Insurance logos that match what the verification team can actually process.
- Outcome and program-length information stated honestly rather than as marketing numbers.
- Staff or alumni stories that read as voluntary lived-experience contributions rather than scripted testimonials, which the CDC identifies as a stigma-reduction strategy when handled respectfully 4.
Each of these is a content decision, not a design flourish, and each removes a question the admissions team would otherwise field on a first call.
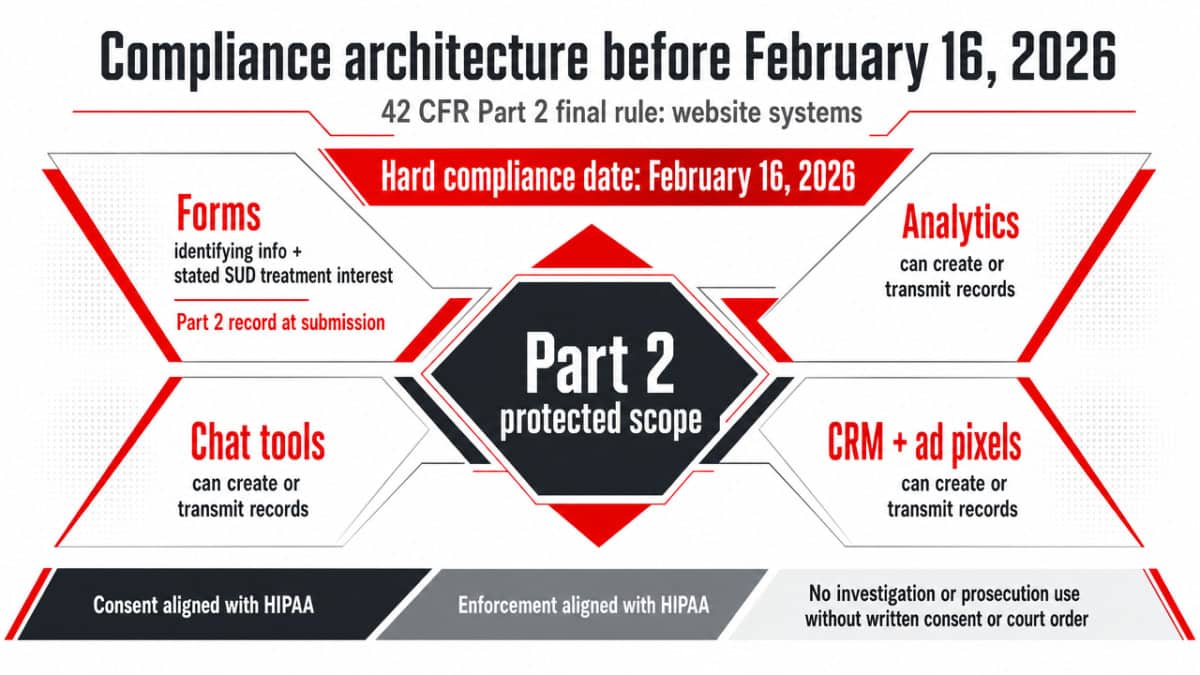
Compliance architecture before February 16, 2026
What the 42 CFR Part 2 final rule changes for website systems
The HHS final rule modifying 42 CFR Part 2 set a hard compliance date of February 16, 2026, aligned consent and enforcement structures with HIPAA, and clarified that SUD treatment records cannot be used to investigate or prosecute a patient without written consent or a court order 10. For treatment center operators, the deadline is not a legal-department problem to file away. It changes how forms, analytics, chat tools, CRM systems, and ad pixels on the website have to be built, because each of those systems can create or transmit records that fall inside Part 2’s protected scope.
Intake forms are the most visible surface. Any web form that captures identifying information alongside a stated interest in SUD treatment is generating a Part 2 record the moment it is submitted. The final rule’s consent framework requires that the disclosure language a visitor sees at the point of submission matches what the facility actually does with the information downstream, including any sharing with affiliated providers or referral partners 10. Generic privacy policies copied from a general medical practice template will not survive an audit on this point.
Analytics and ad pixels are the second exposure. A Google Analytics, Meta, or LinkedIn pixel that fires on a confirmation page after a form submission can transmit information that, combined with the page URL, effectively discloses that an identified user inquired about SUD treatment. The Part 2 alignment with HIPAA penalty structures means that exposure is no longer theoretical 10. Operators should expect to remove standard pixels from all post-submission pages, gate them behind consent, or replace them with server-side measurement that does not transmit identifiers to advertising platforms.
Chat tools and CRM systems are the third. A live chat widget that captures conversation transcripts on a third-party vendor’s infrastructure needs a BAA, and the consent the visitor sees before typing has to align with the new rule’s disclosure requirements. CRM record handling matters equally: a record that lands in the admissions CRM after a form submission carries the same Part 2 protections as a paper intake sheet, which constrains how that record can be exported, shared with marketing automation, or used for retargeting audiences 10. Ad retargeting pixels that build custom audiences from website visitors who reached SUD-specific pages sit in the highest-risk category, because they involve disclosure of identifying information to an external platform without the consent structure the final rule now requires. The systems-affected list is short, but each item touches a workflow the marketing or admissions team uses every day, which is why the February 16, 2026 deadline functions as an operational date rather than a paperwork one.
Operator exposure: which website components carry the most legal risk
Risk on a treatment center website is not evenly distributed. A short list of components concentrates almost all of the legal exposure, and the operator who audits those first removes most of the liability without rebuilding the site.
The highest-exposure component is any form on a page that names a specific substance, condition, or level of care. The combination of a named SUD context and an identifying submission is what triggers Part 2 record status, and the consent language at the point of submission is the document that gets reviewed if the facility is ever questioned about a disclosure. Forms without granular consent capture, or with checkboxes pre-checked by default, are the cleanest finding an auditor or plaintiff’s attorney can produce.
The second-highest exposure is the tracking stack on confirmation and thank-you pages. Operators should treat the URL of a confirmation page as protected information in itself, because the page name often encodes the service the visitor inquired about.
The third concentration of risk sits in vendor relationships the marketing team controls without involving compliance: chat platforms, scheduling tools, call tracking, marketing automation, and any AI tool that processes form content. Each requires a current BAA and a documented data flow showing what leaves the facility’s systems and where it lands. Live chat transcripts and call recordings on third-party infrastructure without a BAA are the kind of finding that turns a single complaint into a systemic enforcement action.
Local presence and the multi-facility question
For operators running multiple facilities under a single brand, the website question is no longer just about conversion design. It is about whether each location reads as a real clinical site with its own staff, license, and program detail, or as a duplicated page with a swapped city name. Search behavior on the visitor side rewards the first and penalizes the second, and the same online health information seeking research that governs the homepage applies at the location level: visitors weigh clarity, credibility, and navigability before they pick up the phone 2.
The location page standard is concrete. Each facility carries its own URL, its own named clinical leadership, its own accreditation marks, its own licensure detail, its own program-level information, and its own insurance verification path. Duplicated copy across location pages signals to the visitor that the operator views the locations as interchangeable, which is the exact opposite of the person-centered, transparency standard that governs the rest of the site 7. It also undermines the structured intake logic of the level-of-care architecture, because a visitor who self-selected a level of care on the main site should land on a location page that confirms the program is actually delivered at that address.
Single-facility operators face a narrower version of the same question: the location page is the homepage, and the trust signals have to do double duty. In both cases, the operational takeaway is that local presence is a content depth problem, not a template problem.
Frequently Asked Questions
What separates a good addiction treatment website from a brochure site?
A brochure site describes services. A clinically functional site routes a visitor toward the correct level of care before the admissions call. That means a persistent call element, a level-of-care selector in primary navigation, transparent program detail, and content that treats the whole person rather than just the substance. The principles map directly to NIDA’s framework on availability, individualized treatment, and multi-need attention 5.
How does the 42 CFR Part 2 final rule change website requirements before February 16, 2026?
The HHS final rule aligns Part 2 consent and enforcement with HIPAA and sets a compliance date of February 16, 2026 10. For website systems, that affects intake forms, analytics and ad pixels on confirmation pages, chat tools, CRM record handling, and any vendor that touches identifying information tied to SUD inquiry. Consent language at the point of submission must match what the facility actually does with the record downstream.
Should telehealth access be featured on the homepage or kept on a separate service page?
Featured. A 2024 meta-analysis of tele-mental health services found generally high user acceptance, indicating prospective patients now expect remote care as a legitimate entry point 8. Burying virtual IOP or telehealth MAT two clicks deep filters out qualified visitors. The level-of-care selector should include a virtual track with the same depth of content as in-person pages: provider, platform, insurance coverage, and scheduling path.
What language and imagery choices reduce stigma for visitors in crisis?
Person-first language replaces “addict,” “clean,” and “substance abuser” with “person with a substance use disorder,” “in recovery,” and “person who uses drugs.” CDC guidance identifies non-stigmatizing language and respectfully framed lived-experience content as evidence-backed strategies for reducing barriers to care 4. Imagery should show real clinicians, real facility interiors, and group settings without dramatized anguish, rather than silhouettes, cliffs, or grayscale despair photography.
How should a treatment website support ASAM level-of-care matching?
The site cannot replicate a clinician’s ASAM assessment, but it can preserve enough structure that visitors arrive at the call already routed. Research on standardized intake in California SUD systems shows that the structure of assessment affects engagement and retention 1. Each level-of-care page should carry a plain-language indication summary, a clear next step to a human, and an honest statement that final placement follows clinical assessment.
Which website components carry the most legal and privacy exposure for operators?
Three components concentrate most of the risk: forms on pages naming a specific substance or level of care, tracking pixels on confirmation and thank-you URLs, and third-party vendors handling chat transcripts, call recordings, or CRM data without a current BAA. Each can transmit identifying information tied to SUD inquiry, which the updated 42 CFR Part 2 framework treats as a protected record requiring explicit consent 10.
References
- Testing a Standard Approach to Match Patients with Addiction to the Level of Care. https://www.ncbi.nlm.nih.gov/books/NBK611652/
- Online Health Information Seeking Behavior: A Systematic Review. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8701665/
- Mental Illness Stigma, Help Seeking, and Public Health Programs. https://pmc.ncbi.nlm.nih.gov/articles/PMC3698814/
- Mental Health Stigma. https://www.cdc.gov/mental-health/stigma/index.html
- Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition). https://nida.nih.gov/sites/default/files/podat-3rdEd-508.pdf
- Table 4.2, Principles of Effective Treatment for Substance Use Disorders. https://www.ncbi.nlm.nih.gov/books/NBK424859/table/ch4.t2/
- Principles of Care in Prevention, Treatment and Recovery. https://www.mass.gov/doc/principles-of-care-in-prevention-treatment-and-recovery/download
- Acceptability of Tele-mental Health Services Among Users: A Systematic Review and Meta-analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC11040906/
- Evidence Brief: Safety and Effectiveness of Telehealth-delivered Mental Health Care. https://www.ncbi.nlm.nih.gov/books/NBK586283/
- Fact Sheet: 42 CFR Part 2 Final Rule. https://www.hhs.gov/hipaa/for-professionals/regulatory-initiatives/fact-sheet-42-cfr-part-2-final-rule/index.html